Case Vignette
A 50M known hypertensive and known diabetic on Insulin developed severe chest heaviness leading to admission at a hospital where a 12L ECG done showed acute inferior wall infarct. The patient also had elevated troponin values at the time. Patient was advised primary PCI at that time but did not give consent and instead opted to be treated medically. Prior to discharge patient was noted to also have Aspirin allergy presenting as facial swelling which was noted to have resolved after anti-histamine administration and discontinuation of Aspirin. Patient had no further reactions while maintained on Clopidogrel, Atorvastatin, Losartan, Carvedilol, ISMN and Trimetazidine.
6 months later post discharge from his episode of MI patient still had episodes of chest heaviness felt mostly everyday, elicited by climbing stairs, lasting 5-10 minutes. These symptoms persisted despite titrate of anti-anginal medication
Patient consulted with a Cardiologist who advised Coronary Angiography with intent to revascularize.
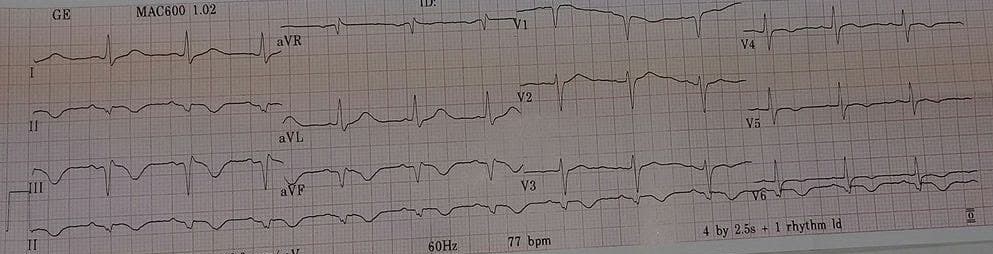
On admission patient was noted to have an essentially unremarkable physical examination except for a displaced apex beat noted most prominent at the 6th ICS left parasternal border. 12L ECG showed regular sinus rhythm left axis deviation and age indeterminate inferior wall infarct and poor R wave progression.
The patient was referred to Allergology service for de-sensitization. However due to limited ICU capacity patient was advised re-admission for Aspirin de-sensitization at another time.
Patient underwent coronary angiography and angioplasty with not untoward events.
Post revascularization patient noted improvement in chest heaviness and improvement in functional capacity, now able to climb stairs without chest heaviness. Patient was sent home on Clopidogrel 75mg tablet once daily and Cilostazol 100mg tab 2 times a day as well as an ACE inhibitor. Beta blockers and maximal dose of statin. Patient is on follow-up with allergology service for planning of desensitization
Guide Questions
1. What is the clinical basis for coronary angiography and angioplasty in this case? What are the latest recommendations on management of Chronic Coronary Syndrome
2. What is the prevalence of Aspirin Hypersenstivity? What are the management options/strategies available in this case?